Giant aneurysm of right sinus of valsalva in a HIV-infected patient with extrapulmonary tuberculosis
———————Soumya Patra,1 Ravindranath K Shankarappa,1 Navin Agrawal,1 Madhav Hegde2
DESCRIPTION
A 46-year-old male patient admitted with fever, cough, chest pain and dyspnoea during the past
7 days. He had a history of unprotected sexual
exposure and was previously undiagnosed for HIV
infection. Chest X-ray revealed bilateral pleural
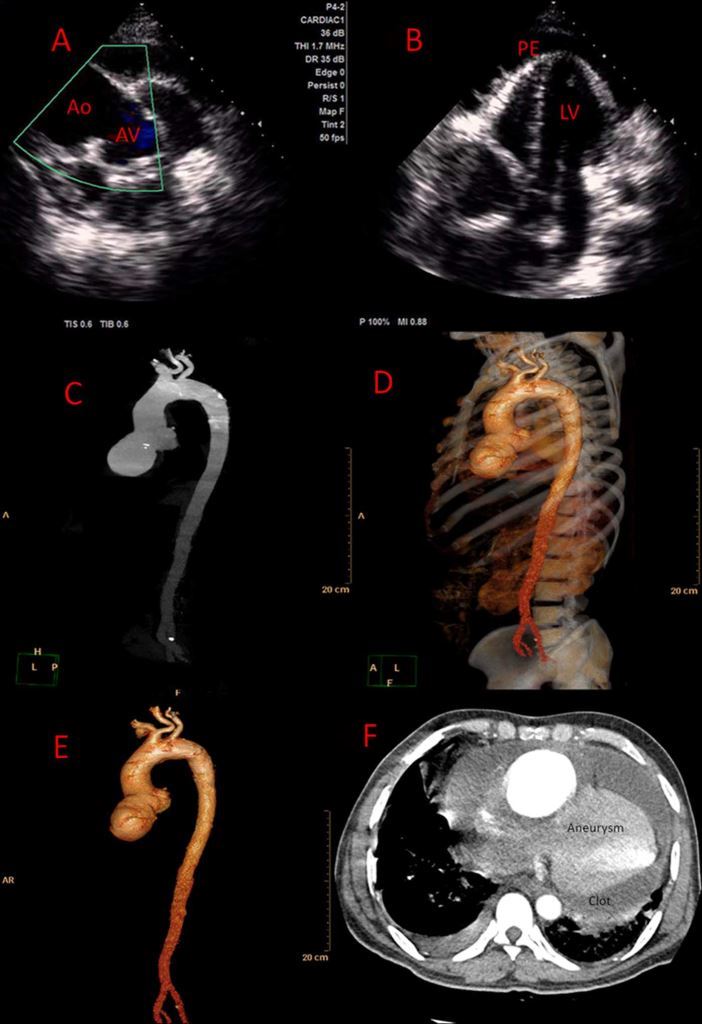
chamber view showed the presence of pericardial effusion, mostly at the left ventricular (LV) apex; (figure 1-F) CT aortogram
and 3D reconstructed images showed a giant aneurysm at the right sinus of valsalva (7.1×8.5 cm) with a clot inside.
effusion along with cardiomegaly. ECG showed sinus tachycardia
with low-voltage complex. Blood investigation revealed
haemoglobin-10.4 g/dL, total leucocyte count 8600/mm3,
platelets 215 000/mm3 with normal liver and renal function
test. 2D echocardiography demonstrated moderate pericardial
effusion, normal biventricular function with dilated and
aneurysmal ascending aorta and mild aortic regurgitation
(figure 1A,B). Pleural fluid aspiration showed straw coloured
fluid with total cell count 600 (lymphocytic), exudative and
very high adenosine deaminase level (ADA 86 U/L).
Serological investigation confirmed the presence of HIV infection.
The patient was started on antitubercular therapy. CT
aortogram confirmed the presence of a giant (7.1×8.5 cm)
aneurysm of the right sinus of valsalva (figure 1C–F). The
patient was unwilling to undergo surgery of the aneurysm of
the right sinus of valsalva.
The differential diagnosis of the aneurysm of the sinus of valsalva
could be Marfan’s syndrome, vasculitis due to tuberculosis,
syphilis and other infectious agents, rheumatological diseases
and HIV-associated vasculitis.1 Only few cases of aneurysm of
the aorta due to HIV infection have been reported in the literature
and the histopathology of the resected aorta revealed a
granulomatous giant cell mesaortitis.2 3 So far this is the biggest
aneurysm associated with HIV.
Learning points
- HIV-associated vasculitis rarely involves the sinus of valsalva-causing aneurysm.
- The differential diagnosis of aneurysm of the sinus of valsalva could be Marfan’s syndrome, vasculitis due to tuberculosis, syphilis and other infectious agents, rheumatological diseases and HIV-associated vasculitis.
- Histopathology of the resected aorta usually revealed a granulomatous giant cell mesaortitis.
Competing interestsNone.
Patient consent
Obtained.
Provenance and peer review
Not commissioned; externally peer reviewed.
REFERENCES
- Boggian K, Leu HJ, Schneider J, et al. True aneurysm of the ascending aorta in HIV disease. Schweiz Med Wochenschr 1994;124:2083–7.
- Mirza H, Patel P, Suresh K, et al. HIV disease an atherosclerotic ascending aortic aneurysm. Rev Cardiovasc Med 2004;5:176–81.
- Choi JB, Yang HW, Oh SK, et al. Rupture of ascending aorta secondary to tuberculous aortitis. Ann Thorac Surg 2003;75:1965–7.
- Submit as many cases as you like
- Enjoy fast sympathetic peer review and rapid publication of accepted articles
- Access all the published articles
- Re-use any of the published material for personal use and teaching without further permission
This is my first comment.
By : Prajyotan B - On : 3/3/2018 9:44:05 AM
This is my first reply
By : Madhav Hegde - On : 3/3/2018 9:44:48 AM
This is my second comment
By : Prajyotan B - On : 3/3/2018 9:44:25 AM