CARDIOVASCULAR FLASHLIGHT
CARDIOVASCULAR FLASHLIGHT
An adult with right aortic arch and dysphagia
Venugopal Ram Rao1, Nagaraja Moorthy2*, Madhav Hegde3, and Manjunath C. Nanjappa2
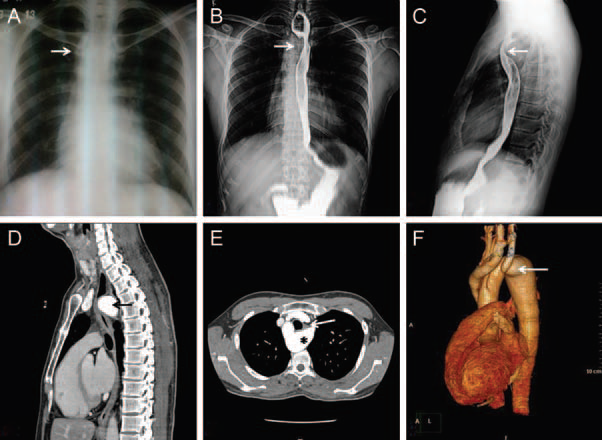
A 38-year-old male presented with history of atypical chest pain and dysphagia. Cardiovascular examination was unremarkable. Electrocardiography and transthoracic echocardiography were normal. Chest radiograph showed right-sided aortic arch (Panel A). Barium swallow was performed, which showed extrinsic compression from right side (Panel B) and from posterior aspect (Panel C) at the level of T4 vertebra. Computed tomography aortogram confirmed right-sided aortic arch with left-sided large aortic diverticulum extending posterior to the oesophagus with marked compression (Panel D and E). There was no compression of the trachea. The volume rendered reconstruction image showed anomalous origin of left common carotid from the ascending aorta and left subclavian artery originating from the diverticulum.
The patient underwent successful surgical resection of the diverticulum with reimplantation of the left subclavian artery to descending thoracic aorta. He made prompt recovery with dramatic improvement in dysphagia. Aortic arch anomalies should be ruled out in patients with dysphagia and right aortic arch irrespective of age at presentation. In individuals with suspected aortic arch anomalies, computed tomography imaging by providing an accurate anatomical diagnosis guides surgical decision-making.
Panel A Chest radiograph showing right-sided aortic arch (arrow). Panels B and C Barium swallow imaging showing extrinsic compression on right side (B) and on posterior aspect (C) of oesophagus (arrows). Panels D and E Computed tomography aortogram showing large aortic diverticula (asterisk) with retroesophageal extension causing marked compression on the oesophagus (arrow). (F) Computed tomography volume rendered aortography showing right-sided aortic arch with anomalous origin of left common carotid from ascending aorta and left subclavian artery arising from aortic diverticulum.
Nice !
By : Pramod Bastawad - On : 3/6/2018 3:11:38 AM
test comment
By : Vishal Patil - On : 4/1/2018 7:48:09 PM