Supra-valvular aortic stenosis in a patient with homozygous familial hypercholesterolaemia
———————Ravindran Rajendran1*, Kikkeri Hemanna Setty Srinivasa1, Kapil Rangan1, Madhav Hegde2, and Naveed Ahmed1
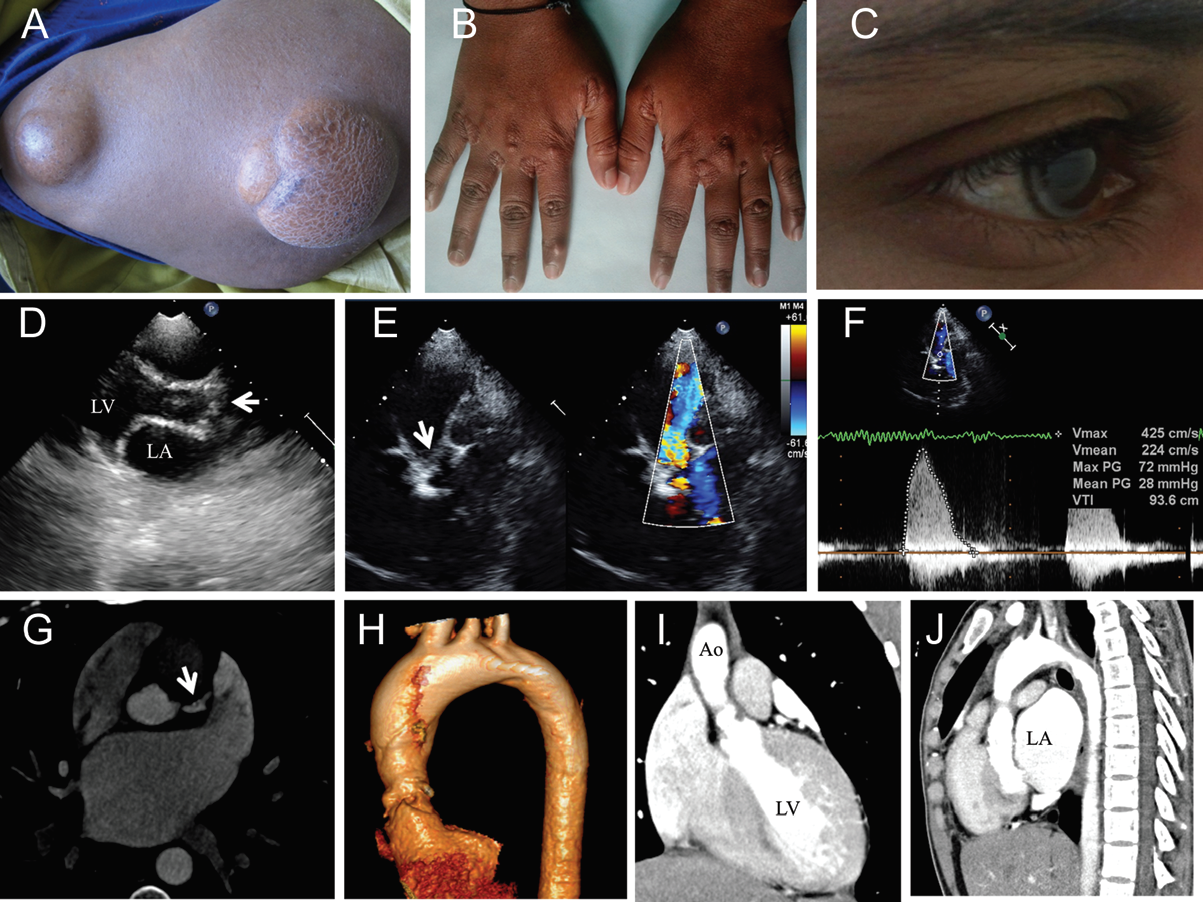
An 18-year-old female was referred for a cardiac murmur before surgical excision of large subcutaneous swellings over bi-lateral trochanteric areas (Panel A). On evaluation they were found to be tendon-xanthomas, that also involved the glutealfolds, finger web-spaces (Panel B), and tendons of the foot. Corneal arcus was also noted (Panel C). Her total cholesterol of 696 mg% and low-density lipoprotein (LDL) cholesterol of 648 mg% were consistent with familial hypercholesterolaemia (FH) type-IIa in the homozygous state. Both parents were having elevated LDL cholesterol but ,300 mg%.
An echocardiogram in the para-sternal longaxis and supra-sternal views (Panels D and E ; Supplementary data online, Video S1 and S2) showed supra-valvular narrowing with mobile aortic cusps. Colour Doppler sample volume over the aortic root from the supra-sternal view showed the onset of turbulence above the level of the aortic valve with a peak Doppler gradient of 72 mmHg (Panel F and Supplementary data online, Video S3). A computerized tomogram (CT) of the aorta showed a tubular narrowing above the aortic valve (Panels H –J). CT coronary angiogram showed calcification of the left-main vessel without any significant stenosis (Panel G).
As she was asymptomatic with a negative exercise treadmill test for inducible ischaemia and a normal CT coronary angiogram she was kept on high-dose statins and ezetimibe. At 6 weeks of follow-up her LDL cholesterol remained high at 620 mg% without any new symptoms. She was advised LDL apheresis and surgery for supra valvular aortic stenosis if symptomdevelops. Though her LDL receptor studies were not available her lipid profile, dyslipidaemic pattern in parents, early onset of xanthomas, and poor response to pharmacotherapy are all consistent with homozygous type II FH. Supra valvular aortic stenosis secondary to large atherosclerotic plaques at the aortic root is an uncommon but a specific association with this form of FH and subsequent risk stratification can be done with currently available noninvasive imaging modalities in asymptomatic patients. Magnetic resonance imaging or transoesophageal echocardiogram can better delineate these plaques.
Thumbnail shared
By : MADHAV HEGDE - On : 4/20/2018 4:45:56 PM