Cor triatriatum sinister - A rare cause of left heart obstruction on MDCT
———————Madhav Hegde*1, and Chanabasappa V Chavadi2
ABSTRACT
Cor triatriatum sinister is a very rare congenital abnormality, with autopsy reported incidence of 0.1 % to 0.4%. Here it is subdivision of the left atrium into proximal and distal chamber by a fibromuscular membrane. Our case is unique in that it is the first case report of 64-slice multi detector computed angiography revealing cor triatriatum with least common associations of PDA, VSD and polysplenia. The etiopathogenesis, advantages of MDCT for detecting associated anomalies and prognosis are discussed
Keywords: Cor triatriatum sinister, Shone’s complex, Congenital Heart Disease, Multi Detector Computed Tomography (MDCT).
1. Introduction
Cor triatriatum sinister is a sporadic congenital heart anomaly characterized by compartmentalization of left atrium into two chambers by a fibromuscular membrane to form a triatrial heart. The proximal (posterior-superior) chamber receives the pulmonary venous drainage; the distal (anterior-inferior) chamber contains the mitral valve and the left atrial appendage. These chambers are in communication via one or more fenestrations in the membrane. Though, the manifestation in neonates is the most common presentation, few of them get detected in adulthood incidentally. Recent advances in cardiovascular imaging, encompassing echocardiography and computed tomography (CT) have made the diagnosis of cor triatriatum and associated anomalies easier [1,2]. In this backdrop, we report a rare case of cor triatriatum sinister completely characterized by 64-slice CT angiography and echocardiography.
2. Case ReportMale child aged 1.5 years presented with feeding difficulty, poor weight gain, symptoms of pulmonary venous obstruction, congestive heart failure. Equivocal soft murmur
was heard. Child had tachypnea and with decreased peripheral pulses.
The child was subjected to transthoracic echocardiography which displayed a membranous Ventricular Septal Defect (VSD), coarctation of aorta and a membrane like echogenic focus (further characterization was difficult due to poor echocardiography window) in relation to left atrium. With this constellation of findings differentials of Cor triatriatum and partial Shone’s complex were considered.
Further, in view of complex cardiac anomalies CT angiography was performed. Multi detector computed tomography (MDCT) study depicted a thick membrane (Figure 1A-1E) in left atrium with its compartmentalization. Aortic coarctation, membranous VSD, PDA, persistent left SVC (draining into coronary sinus) were well demonstrated. Two normal papillary muscles were seen. In addition polysplenia (Figure 2A- 2D) was seen in the absence of signs of heterotaxy syndrome. Based on the above findings diagnosis of cor triatriatum sinister was concluded.
Parents were counselled about the complex nature of the disease and the surgical options. Parents refused surgical options.
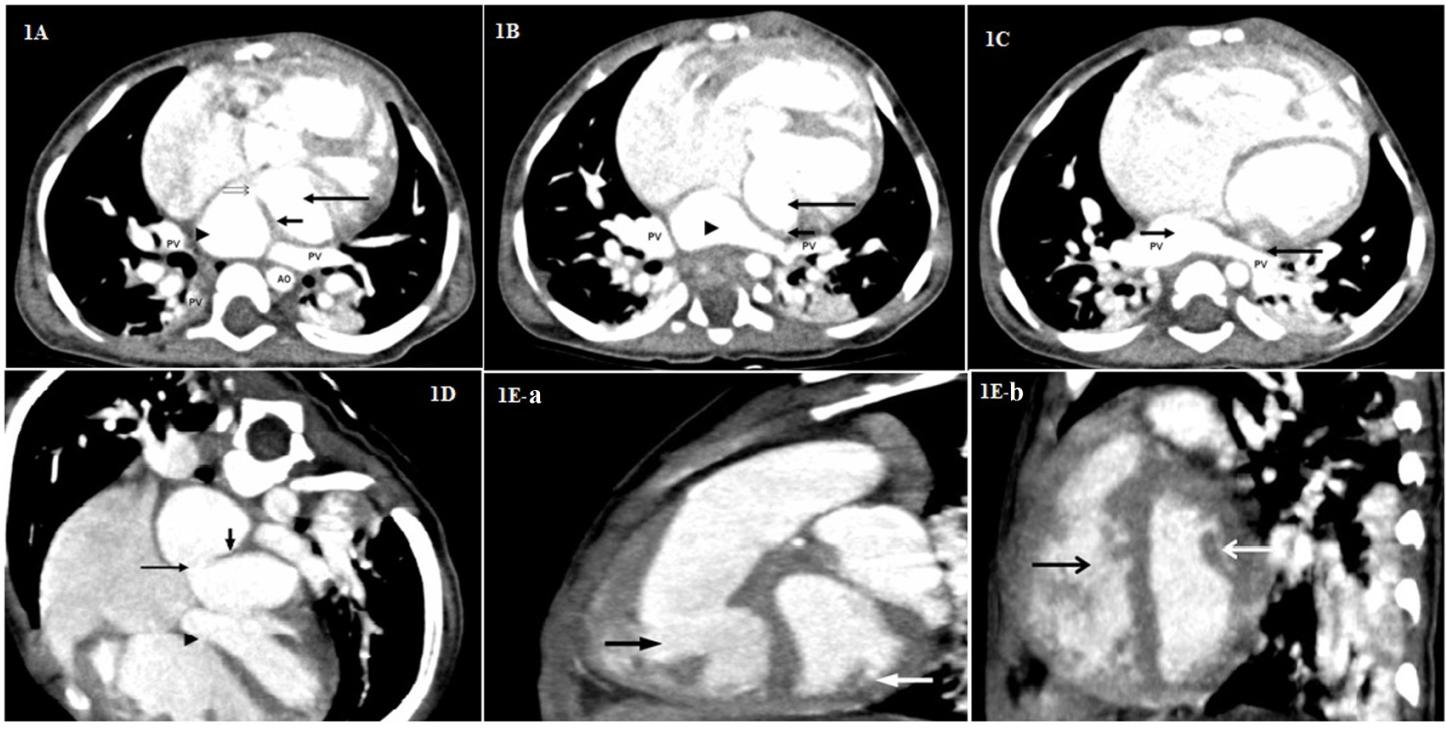
Figure 1A: Transverse source image showing thick septations (short arrow), anterior (long arrow) and posterior (arrow head) chamber, fenestration (double arrow) in the membrane. PV-Pulmonary Vein, AO-descending thoracic aorta.
Figure 1B: Transverse source image showing anterior (long arrow), posterior (arrowhead) Chamber, intra atrial membrane (short arrow) in cor triatriatum sinister. PV-Pulmonary Vein
Figure 1C: Transverse source image showing membrane (long arrow) in left atrium, posterior chamber (short arrow) of left atrium receiving pulmonary vein (PV).
Figure 1D: Horizontal long axis (4 chamber) reconstructed image depicting membrane (short arrow), fenestration (long arrow), ventricular septal defect (arrow head).
Figure 1E-a & Fig 1E-b: Saggital reconstructed images demonstrating normal papillary muscles (white arrow) excluding the possibility of Shone’s complex. Black arrow indicates right ventricular cavity.
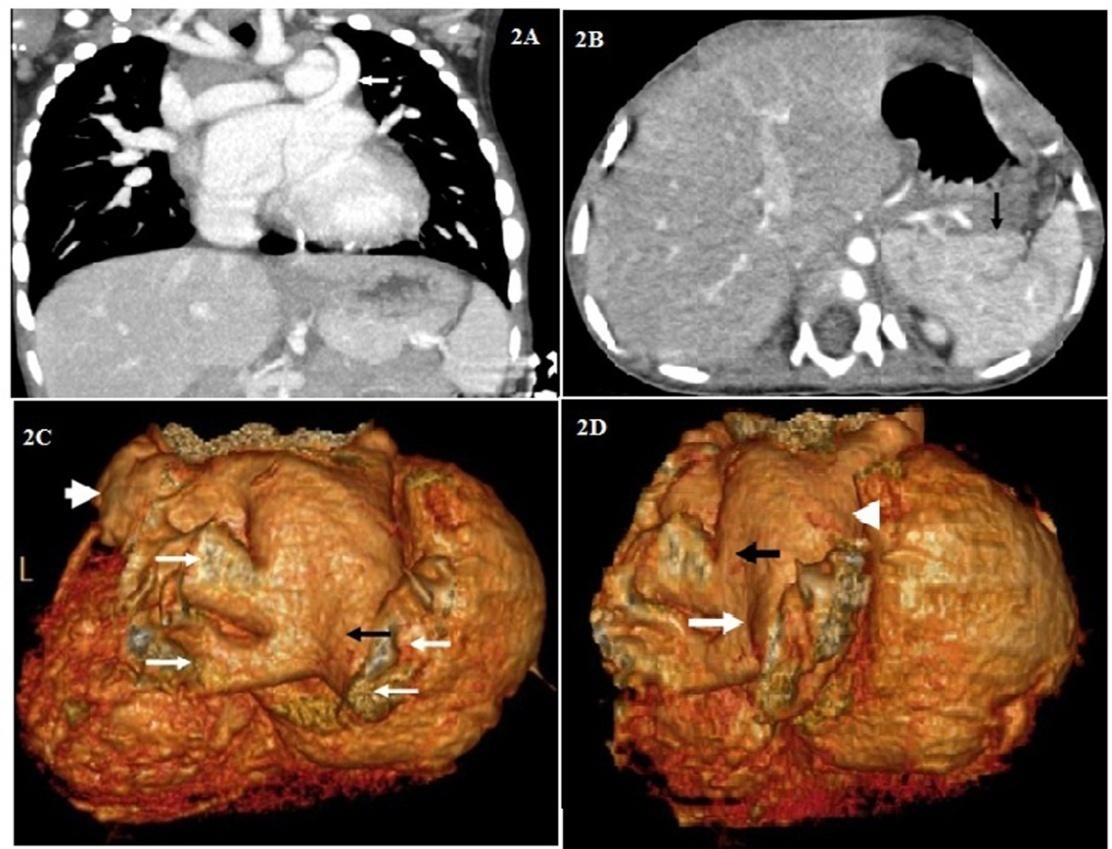
Figure 2A: Coronal reconstructed image with arrow indicating left persistent SVC draining into coronary sinus.
Figure 2B: Transverse source image showing polysplenia (arrow).
Figure 2C: Volume rendered image viewed from posterior aspect showing posterior chamber (black arrow)of left atrium, pulmonary veins ( long white arrows) draining into posterior compartment of left atrium, left atrial appendage (short white arrow) of anterior (distal) chamber of left atrium-left of the patient (child).
Figure 2D: Volume rendered image viewed from posterolateral aspect demonstrating posterior (long white arrow) and anterior (white arrowhead) chamber of septated left atrium with black arrow indicating the region of fenestration in the membrane.
Cor triatriatum, a rare cardiac anomaly first reported by Church (1868), which is described as a partition of left atrium into proximal and distal chambers, by a fibromuscular membrane. The severity of the lesion depends on the size, number of septations and transmembrane flow. The incidence of Cor triatriatum ranges between the 0.1% and 0.4% of all congenital cardiac defects [3,4].
The basic classification of cor triatriatum was framed by Loefller in 1949 [5] .The defect is classified into three types based on the anatomical feature of the defect like number and size of fenestrations in the fibromuscular membrane dividing the left atrium. Type 1: Defect having no opening, Type 2: Defect having one or more small openings and Type 3: Defect having single, large opening [5]. Apart from the Loefller classification the other reported forms of Cor triatriatum were based on the fenestration shape [6] and presence of Atrial Septal Defect (ASD) [7]. Cor triatratum sinister in paediatrics is commonly associated with congenital cardiac lesions like ostium secundum atrial septal defect and anomalous pulmonary vein return [8]. Our case is associated with VSD, persistent left SVC, PDA, polyspenia.
Since the end of the 20th century, echocardiography has been the mainstay of imaging for the diagnosis of cor triatriatum [9,10]. The echocardiogram includes study of the 2D pattern of the membrane, analysis of turbulent flow on color Doppler and determination of any gradient across the membrane on continuous wave Doppler. Furthermore, the existence of co morbid congenital cardiac anomalies can be studied by echocardiography. A retrospective review study showed that transthoracic echocardiography has 98% accuracy in diagnosis cor triatriatum [11].Currently, advanced sophisticated imaging techniques like cardiac CT have been extensively employed for the non invasive evaluation of coronary artery disease. Mounting clinical evidences report the diagnosis of cor triatriatum using CT [12,13]. Our case is unique in that it is the first report of 64- slice multi detector computed angiography revealing cor triatriatum with least common associations of PDA, VSD and polysplenia. Studies reveal that cardiac CT has potential benefits with safety and economical aspects when compared to the conventional coronary angiography in the non-invasive evaluation of coronary artery disease [14]. In addition, high spatial and temporal resolutions images in cardiac CT provide information regarding cardiac anatomy, wall motion and myocardial perfusion. In this regard, our case demonstrates the utility of CT in diagnosing the underlying complex anatomic abnormalities in cor triatriatum.
4. ConclusionAlbeit, echocardiograph is used in the diagnosis of cor triatratum sinister, advanced techniques like MDCT and
MR are highly recommended for the complete and accurate characterization of the usually complex anomalies. Considering the nature of complex anatomical and physiological abnormalities of these cardiac defects, MDCT is a mandatory investigation if major therapeutic interventions (percutaneous or surgical) are contemplated.
References- Church WS. Congenital malformation of the heart: Abnormal septum in the left auricle. Trans Pathol Soc Lond 1868; 19:188-90.
- Van Praagh R, Corsini I. Cor triatriatum: Pathologic anatomy and a consideration of morphogenesis based on 13 postmortem cases and a study of normal development of the pulmonary vein and atrial septum in 83 human embryos. Am Heart J 1969; 78:379–405.
- Niwayama G. Cor triatiatum. Am Heart J 1960; 59:291-317.
- Jorgensen CR, Ferlic RM, Varco RL, Lillehei CW, Eliot RS. Cor triatriatum. Review of the surgical aspects with a follow-up report on the first patient successfully treated with surgery. Circulation 1967; 36:101-7.
- Loeffler E. Unusual malformation of the left atrium: Pulmonary sinus. Arch Pathol 1949; 48:371-6.
- Marin-Garcia J, Tandon R, Lucan RV Jr, Edwards JE. Cor triatriatum: Study of 20 cases. Am J Cardiol 1975; 35: 59-66.
- Lam CR, Green E, Drake E. Diagnosis and surgical correction of 2 types of triatrial heart. Surgery 1962; 51:127-37.
- Humpl T, Reineker K, Manlhiot C, Dipchand AI, Coles JG, McCrindle BW. Cor triatriatum sinistrum in childhood. A single institution’s experience. J Cardiol 2010; 26: 371–6.
- Patel AK, Ninneman RW, Rahko PS. Surgical resection of cor triatriatum in a 74 year old man. Review of echocardiographic findings with emphasis on Doppler and transesophageal echocardiography. J Am Soc Echocardiogr 1990; 3:402-7.
- Buchholz S, Jenni R. Doppler echocardiographic findings in 2 identical variants of a rare cardiac anomaly, “subtotal”cor triatriatum: A critical review of the literature. J Am Soc Echocardiogr 2001; 14:846-9.
- Alphonso N, Norgaard MA, Newcomb A, d’Udekem Y, Brizard C, Cochrane A. Cor triatriatum: Presentation, diagnosis and long-term surgical results. Ann Thorac Surg 2005; 80:1666-71.
- Tanaka F, Itoh M, Esaki H, Isobe J, Inoue R. Asymptomatic cor triatriatum incidentally revealed by computed tomography. Chest 1991; 100:272-4.
- Chen K, Thng CH. Multislice computed tomography and two-dimensional echocardiographic images of cor triatriatum in a 46-year-old man. Circulation 2001; 104:2117.
- Chow BJ, Hoffman U, Nieman K. Computed tomographic cardiac angiography: An alternative to invasive coronary angiography. Can J Cardiol 2005; 21:933-40.