Images in cardiovascular medicine
Misdiagnosis of subclavian
artery stenosis: the importance
of dynamic manoeuvre
Rajiv Ananthakrishna,1 Madhav Hegde2
A 27-year-old man was referred for endovascular intervention to the left subclavian artery. There was no history of giddiness or claudication pain in the upper extremities. On examination, the left upper limb pulses were feeble. Blood pressure was 160/ 90 mm Hg in the right upper limb and 110/90 mm Hg in the left upper limb. There was a bruit in the left supraclavicular area. Routine blood investigations, including inflammatory markers, were normal. CT angiography revealed a discrete narrowing of the third part of the left subclavian artery (figure 1). A diagnosis of aorto-arteritis was considered, based on American College of Rheumatology criteria. However, there was no thickening of the vessel wall. The patient was re-evaluated. Wright’s hyperabduction test was performed.1 The signs disappeared with the arm in an adducted position and were reproduced in the abducted position. Repeat CT in the adducted position showed no evidence of subclavian obstruction (figure 2). A diagnosis of dynamically induced arterial thoracic outlet syndrome was made.
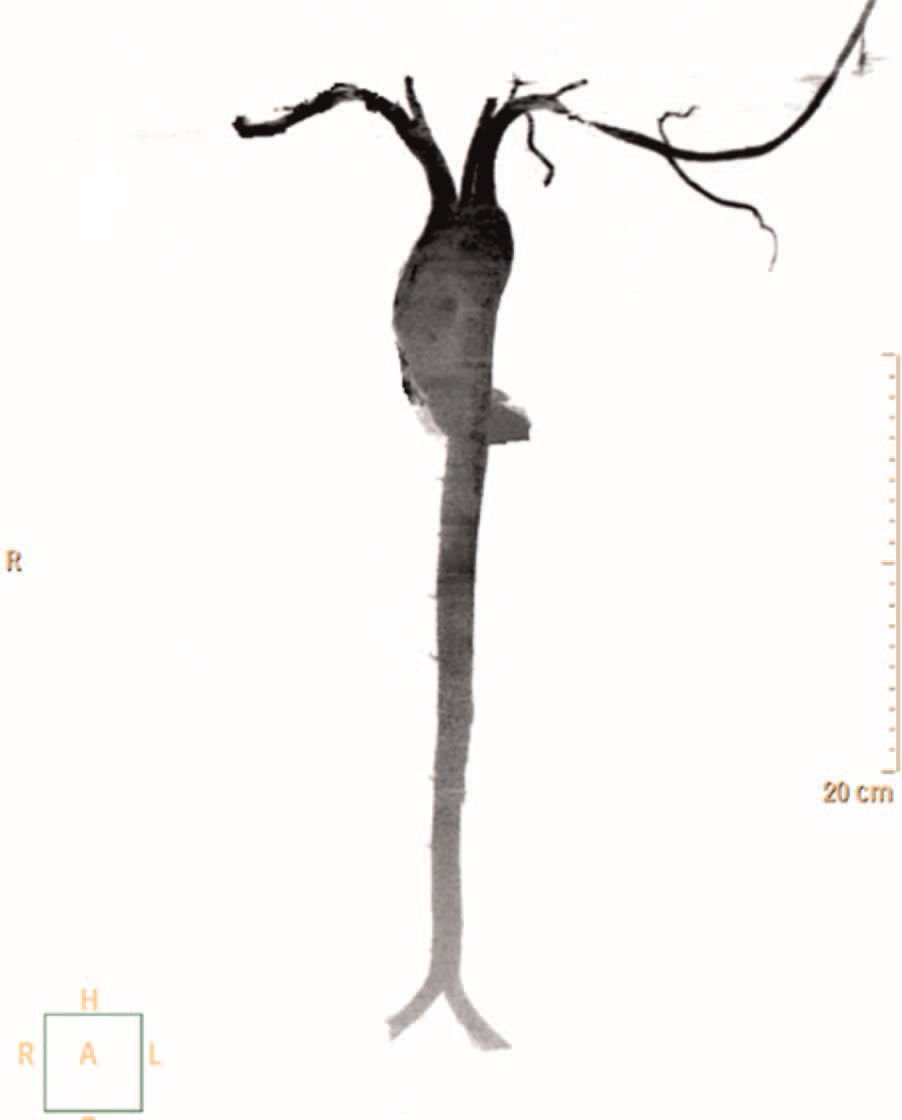
Figure 1 CT angiogram showing discrete stenosis in the third part of the left subclavian artery.

Figure 2 Repeat CT angiogram with the arm in the adducted position, revealing no evidence of subclavian artery obstruction.
The differential diagnoses involving stenosis of the third part of the subclavian artery include aorto-arteritis, cervical rib, elongated C7 transverse process, exostosis or tumour of the first rib or clavicle, post-traumatic/postoperative fibrous scarring and congenital muscle abnormalities. In the absence of overt causes, dynamic manoeuvres such as Wright’s test are useful in demonstrating extrinsic compression of the subclavian artery. Repetitive microtrauma causes fibrosis and spasm of scalene muscles, leading to elevation of the first rib and consequently impingement on neurovascular structures. This report highlights the significance of dynamic manoeuvres in appropriate clinical setting.
Contributors Both authors were involved in the patient workup and manuscript
preparation.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; not externally peer reviewed
REFERENCE
1 Wright IS. The neurovascular syndrome produced by hyperabduction of the arms. Am Heart J 1945;29:1–19.Thumbnail shared
By : MADHAV HEGDE - On : 4/20/2018 4:43:18 PM
Title is wrong And next to thumbnail-in the title-plse remove the name of the author
By : MADHAV HEGDE - On : 4/22/2018 1:22:16 PM