Acute pulmonary embolism being the first presentation of undetected HIV infection:report of two cases
———————S Patra, Q1 CM Nagesh, B Reddy, BC Srinivas, CN Manjunath and M Hegde
INTRODUCTION
Infection with the human immunodeficiency virus (HIV) is now a major health problem worldwide and a chronic disease.1 In recent literature, the relationship between HIV infection and cardiovascular disease has been addressed.1 Studies have shown an increased risk of arterial and venous vascular diseases in HIV patients.2 HIV infection has been recognized as a prothrombotic condition and has been proven by a large number of studies with a reported venous thromboembolism (VTE) frequency among HIV patients ranging from 0.19% to 7.63%/year, whereas frequency of pulmonary embolism (PE) is about 0.26%.3 HIV infection is associated with a 2–10 -fold increased risk of venous thrombosis in comparison with a general population of the same age.2 Some risk factors demonstrated a strongest association with VTE such as, low CD4 in the presence of clinical AIDS, protein S deficiency and protein C deficiency or malignancy.2 But in asymptomatic patient presenting as acute PE as first presentation is extremely rare with single case reported so far.4 We are presenting two cases who were admitted for acute PE and later found to be HIV positive.
CASE REPORT
Case 1
A 44 years old male patient admitted into our hospital for acute onset dyspnoea of five days duration. He has also given the history of significant weight loss in the last three months and had history of exposure. On examination, his oxygen saturation was 90% in room air along with he had tachycardia (heart rate 120/min), tachypnoea (respiratory rate 28/min) and normal blood pressure (BP) of 110/76 mmHg. Cardiac and other system examinations did not revealed any other abnormality.
Haematological parameters and coagulation profile were within normal limit (Hb 11.3 g/dL; total leukocyte count (TLC) 5800/cm; platelet count – 25,4000/cm). Chest X-ray (CXR) was normal and electrocardiogram (ECG) showed sinus tachycardia with S1Q3T3 pattern and T wave inversion in mid-chest leads. D-dimer was found to be positive with 1.26 mg/L (normal value – ,0.6 mg/L) and cardiac troponin T assay was within normal limit. Echocardiography at admission showed dilation right atrium (RA) and right ventricle (RV) with pulmonary artery systolic pressure (PASP) of 64 mmHg. As he had acute onset dyspnoea, positive d-dimer test and electrocardiogram and echocardiographic evidences suggestive of acute PE, he was treated with injection of streptokinase (STK) 2.5 lacs unit bolus and followed by 1 lac unit/hour infusion. Routine serological investigation, which is sent to all admitted patients as a protocol in our hospital, showed HIV-positive in this case. Computed tomography pulmonary angiogram (CTPA) done after 24 hours of giving injection STK was within normal limit. Doppler venography was also within normal limit. After 24 hours, PASP was come down to only 24 mmHg and both tachycardia and tachypnoea was settled. Injection STK was stopped after 24 hours without any complication. He was put on oral anticoagulant and referred to HIV centre for antiretroviral therapy (ART). This patient belonged to World Health Organization (WHO) clinical stage II of HIV infection due to presence of moderate unexplained weight loss with CD4 count was 375/mm3.
Case 2
A 48 years old male patient with diabetes mellitus and old pulmonary tuberculosis was admitted in our hospital due to having dyspnoea on exertion for 10 days along with chest pain. On examination, his oxygen saturation in room air was 92% along with he had tachycardia (heart rate- 124/min), tachypnoea (respiratory rate 24/min) and hypotension
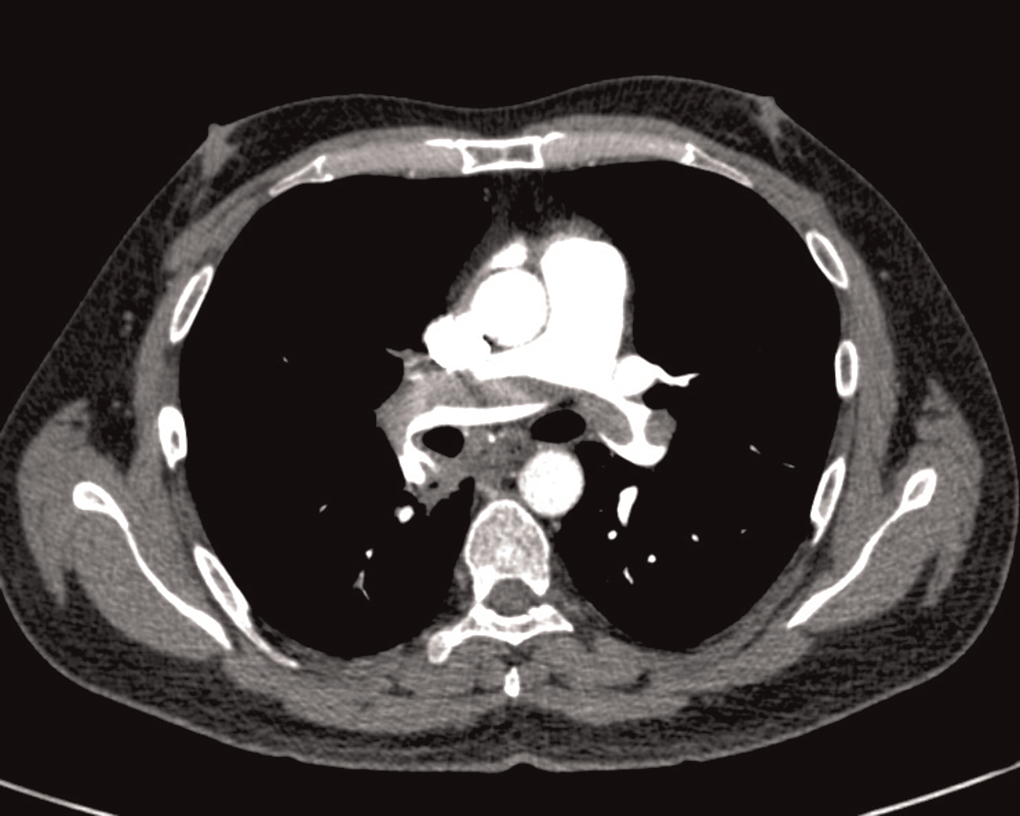
Figure 1 Computed tomography pulmonary angiogram showed thrombi in both pulmonary arteries suggestive of acute pulmonary embolism .
(BP 90/70). On cardiac system examination he had engorged neck vein. Other systems were found to be normal. He had normal CXR and ECG showed sinus tachycardia, S1Q3T3 with features of right ventricular hypertrophy and right axis deviation. Routine haematological parameters and coagulation profile were within normal limit (Hb 15.2 g/dL; TLC 8760/mm3; Platelet count 45,2000/mm3). Both d-dimer (2.69 mg/L) and cardiac troponin T was positive. Echocardiography at admission showed both RA and RV dilation with features of RV dysfunction and PASP of 72 mmHg. In this case CTPA was done in emergence which showed thrombi in both right and left pulmonary artery (Figure 1). Doppler venography was found to be normal. He was also give injection of STK for 48 hours with no complication. In this case also patient was incidentally diagnosed as having HIV infection. The PASP had come down to 42 and 30 mmHg at 24 hours and seventh day of treatment. Patient was discharged and referred to HIV centre after starting oral anticoagulant. This case belonged to WHO clinical stage I (asymptomatic) of HIV infection with CD4 count was 521 cell/mm3.
So in both the cases, acute PE was the first presentation of HIV infection and HIV infection was diagnosed incidentally on routine investigation. They were undiagnosed before admission to our hospital.
DISCUSSION
Patients with HIV infection have an increased risk of thrombosis, with an incidence as high as 8% as opposed to non-HIV-infected individuals.5 Some study reveals up to a 43% increase in risk of developing a PE, 10% increase in developing a DVT in an HIV-infected individual over the nine-year study period after adjusting for age.6 The causes of thrombosis in patients with HIV infection include opportunistic infection (mainly that due to cytomegalovirus), related malignancies and receipt of drugs (e.g. protease inhibitors, abacavir and megestrol acetate), injection drug use.5 The increased risk of DVT in HIV-infected patients could be related to increased levels of procoagulant factors with acquired haematological disorders (protein S and protein C deficiency, protein C resistance
with factor V Leiden mutation, lupus anticoagulant positivity and aCL) and HIV infection itself.6 Additionally, there is a significant correlation between thrombotic disease and a CD4þ cell count of ,200 cells/mm3.7 Endothelial cells could play an important role in the activation of the coagulation cascade during HIV infection.5 Another triggering factor of the coagulation cascade in HIV patients could be stimulation of micro particles.6 The increased risk of DVT during HIV infection could also be related to the impaired functioning of several important anticoagulant proteins.5 In HIV-infected patients with thrombosis, lowered levels of antithrombin (AT) were reported. AT is the most important physiological inhibitor of activated coagulation factors (IIa, IXa, Xa, Xia and XIIa).7 Except one case,4 all other reported cases patients were having advance HIV infection and VTE is common in that situation. But in our case HIV was diagnosed incidentally after admission for acute PE and both the cases had normal coagulation profile.
In the search of suspected pulmonary emboli, basic imaging investigations may support clinical suspicion and exclude alternative diagnoses. Chest radiographic appearances may be relatively non-specific and often confusing. CTPA is the imaging modality of first choice.4 One of our patients had CTPA features of PE but in another case CTPA was normal though it was done 24 hours after receiving injection STK. Though first case had significant weight loss but other case did not have any feature of HIV infection. Treatment of PE in cases with HIV also same as patient without HIV infection. As both the patients had features of RV dysfunction, so they were treated with injection of STK.8 We have treated both the cases with injection of STK and both the patients showed improvement with this treatment. Oral anticoagulant was also started. Some ART can have interaction with oral anticoagulant. 7 But in our cases ART was not started and they were referred to HIV centre.
Though PE is usually seen in advanced HIV infection but in any patient presented with acute PE even without any symptoms of HIV or acquired immunodeficiency syndrome, HIV infection has to be ruled out. Treatment with fibrinolytic agent like injection of STK should be given if there is presence of RV dysfunction of hypotension which is same as patient without HIV infection. If patients need ART then frequent monitoring is needed while patient is on oral anticoagulant.
Contributors: SP, NCM, BR & BCS diagnosed the cases, reviewed the literatures and drafted the manuscript. BCS & CNM corrected the manuscript. MH helped in doing CT pulmonary angiogram. All authors approved the final version of the manuscript.
REFERENCES
- Malek J, Rogers R, Kufera J, Hirshon JM. Am J Emerg Med 2011;29:278–82
- Nagaraja V, Terriquez JA, Gavini H, Jha L, Klotz SA. Pulmonary embolism mimicking pneumonia in a HIV patient. Case Report Med 2010;2010:394546
- Howling SJ, Shaw PJ, Miller RF. Acute pulmonary embolism in patients with HIV disease. Sex Transm Infect 1999;75:25–9
- Germano N, Mendonc¸a P, Murinello A. Pulmonary embolism associated to HIV infection. Rev Port Pneumol 2005;11:407–12
- Asherson RA, Go´mez-Puerta JA, Marinopoulos G. Recurrent pulmonary thromboembolism in a patient with systemic lupus erythematosus and HIV-1
- Bibas M, Biava G, Antinori A. HIV-associated venous thromboembolism. Mediterr J Hematol Infect Dis 2011;3:e2011030
- Klein SK, Slim EJ, de Kruif MD, et al. Is chronic HIV infection associated with venous thrombotic disease? A systematic review. Neth J Med 2005;63:129–36
- Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141(Suppl.):e419S–94S