Hirayama disease
———————Chanabasappa V. Chavadi, Goutam Jasti, Madhav Hegde1, Anand Venugopal
A B S T R A C T
INTRODUCTION
Hirayama disease (HD) is a rare cervical myelopathy also referred as monomelic amyotrophy, juvenile muscular atrophy of the distal upper limb, benign focal amyotrophy, and juvenile asymmetric segmental spinal muscular atrophy. HD primarily affects young men in the second to third decades of life.
CASE REPORT
A 24-year-old adult male presented with a 4-year history of slowly progressive asymmetric weakness in the hands and forearm, with right being affected greater than left. Neurologic examination revealed atrophic changes in the muscles of the hands and forearm, except the brachioradialis, giving a characteristic appearance of oblique amyotrophy. Furthermore, there was partial loss of function at the biceps and shoulders muscles suggestive of C4 and C5 myotomes involvement. Subtle irregular tremulous movements in the right fingers were noted. Sensation was well preserved. No extra pyramidal signs, Horner sign, or abnormalities in sweating and urination were noted. Electromyography changes pointed toward an
| Access this article online | |
| Quick Response Code: |
Website: www.ijns.in |
|
DOI: *** |
|
active denervation change. Based on the clinical findings, the differential diagnoses included a restricted form of motor neuron disease (monomelic muscular atrophy), a limited form of multifocal motor neuropathy, and chronic radiculopathy.
The cervical spine radiographs were normal. Routine magnetic resonance image (MRI) [Figure 1a] revealed spinal cord atrophy from C4-C5 to C6-C7 disc levels, but without history of trauma or ischemic insult and with no evidence of compressive lesion or osteophyte, cord atrophy appeared nonspecific. Thinning of the spinal cord is evident as reduction in the anteroposterior diameter of the spinal cord with myelomalacia more prominent in right hemicord [Figures 1a, 3a and 3b].
Given the young age of patient and focal spinal cord atrophy, a dynamic evaluation of the cervical spine with flexion and extension was performed. MRI during neck flexion on T2-weighted images [Figure 1b and c] revealed anterior displacement of the posterior dura with epidural flow voids and compression of the spinal cord. Flexion pre and postcontrast T1 MRI in midline sagittal plane [Figure 2a and b] revealed enhancement in posterior epidural space suggestive of enhancement of epidural plexus. Axial postcontrast T1 flexion MRI [Figure 3c and d] demonstrates thinning of the spinal cord, more prominent in right hemicord with posterior epidural enhancement. On extension in postcontrast T1 [Figure 2c], the posterior epidural space and its enhancement disappeared consequent to posterior displacement of posterior dura, also the cord compression was relieved.
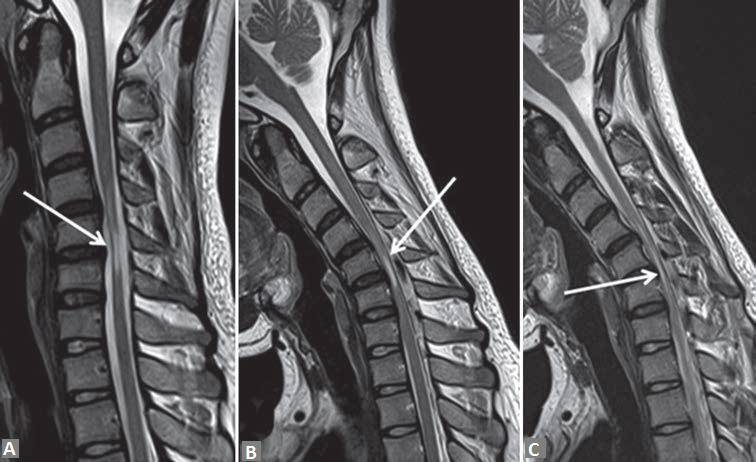
Figure 1: T2-weighted sagittal magnetic resonance imaging in neutral position (a) and in neck flexion (b and c) demonstrate anterior displacement of the posterior dura (white arrow in b) with thinning of the spinal and myelomalacia (white arrow in a and c). Epidural fl ow voids posterior to dura also seen (b and c)
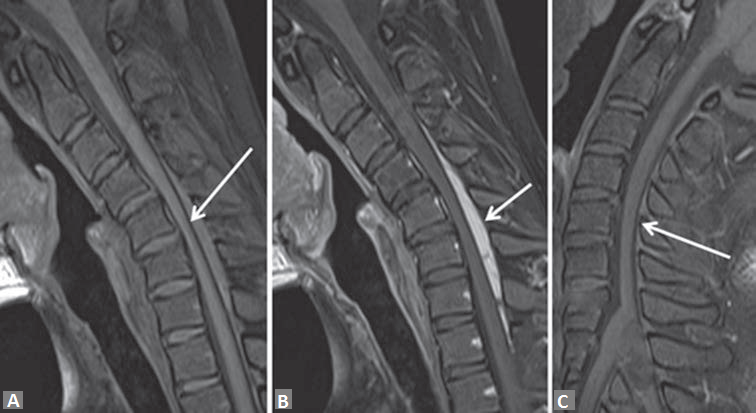
Figure 2: T1-weighted sagittal noncontrast flexion (a) and dynamic pre and postcontrast flexion T1-weighted (b and c) magnetic resonance imaging reveals the anteriorly posterior dura (white arrow in a), enhancement in posterior epidural space (white arrow in b) suggestive of enhancement of epidural plexus. In postcontrast extension T1-weighted sagittal magnetic resonance imaging (c) the posterior epidural space and its enhancement disappeared consequent to posterior displacement of posterior dura, also the cord compression was relieved
Forward displacement of the posterior dura mater, epidural enhancement and compression of the spinal cord as seen in flexion MRI is characteristic of HD. A diagnosis of HD was made and patient was advised a cervical collar. A repeat MRI after 6 months and 18 months revealed stable cervical myelopathy.
DISCUSSION
Hirayama disease is a benign disorder with insidious onset involving the cervical spinal cord. A stable stage is usually reached after a steadily progressive course
occurring mainly in young males between the ages of 15 and 25 years.[1,2] HD is manifested by hand weakness and fatigue, followed by cold paresis, tremors and atrophy with slow progression.
The tight dural canal in flexion can be explained by anteriorly displaced dura, caused by a disproportional growth between the individual’s vertebral column and the dural canal.[3] Spinal dura mater is attached to the vertebral bodies at two places: One at the foramen magnum and dorsal surface of C2-C3 and the another at the coccyx. Rest of the dura mater is loosely suspended
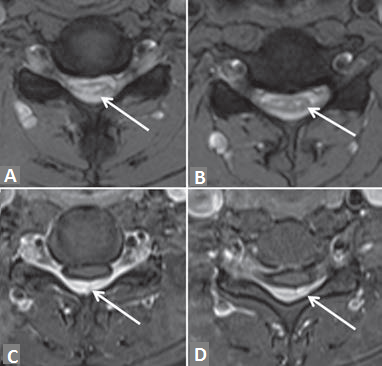
Figure 3: T2-weighted axial flexion magnetic resonance imaging (a and b) and postcontrast T1-weighted (c and d) demonstrates thinning of the spinal cord with myelomalacia (white arrow in a and b), more prominent in right hemicord with complete eff acement of the cerebrospinal fluid space surrounding the cord. Enhancement of posterior epidural space in postcontrast T1-weighted images (white arrow in c and d)
like a sac inside the vertebral column enclosed by
epidural fat, venous plexus, and loose connective tissue.[4]
When neck is flexed, the cervical cord is longitudinally
stretched. In HD, the lower cervical cord moves forward
in flexion and contacts the posterior surface of the
vertebrae; the lower cervical cord becomes flattened
at contact point. In addition, the posterior wall of the
dural tube moves forward, the posterior epidural space
expands forming a crescent-shaped mass in the posterior
epidural space formed by the congestion of posterior
internal vertebral venous plexus.[5] This compression
may cause microcirculatory disturbances in the territory
of the anterior spinal artery or in the anterior portion
of the spinal cord. The chronic circulatory disturbance
resulting from repeated or sustained flexion of the neck
may produce necrosis of the anterior horns, which are
most vulnerable to ischemia.[6]
Magnetic resonance imaging studies in neck flexion will show the forward displacement of the posterior wall and a well-enhanced crescent-shaped mass in the posterior epidural space of the lower cervical canal. [7] Atrophy of the lower cervical cord in a neutral position, abnormal cervical curvature (straight or kyphotic), loss of
attachment between the posterior dural sac and subjacent lamina are the classical findings on MRI. Early recognition of this condition is necessary, because simple postural changes such as avoidance of neck flexion by cervical collar can stop the progression of this disease in early stages. Low pillows are recommended. Although duroplasty, anterior cervical decompression and reconstructions with tendon transfers have yielded encouraging results in selected patients.[8]
CONCLUSION
Hirayama disease is a rare self-limiting disease. Diagnosis is possible when suspected on routine neutral MRI, as a cause of spinal cord myelopathy in absence of canal narrowing, which should prompt to perform exaggerated flexion MRI with contrast. Use of a simple cervical collar, has been shown to halt the progression of the disease as seen in our case.
REFERENCES
- Hirayama K. Non-progressive juvenile spinal muscular atrophy of the distal upper limb [Hirayama’s disease]. In: De Jong JM, editor. Handbook of Clinical Neurology. Vol. 15. Amsterdam, the Netherlands: Elsevier; 1991. p. 107-20.
- Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH. Hirayama disease: MR diagnosis. AJNR Am J Neuroradiol 1998;19:365-8.
- Kikuchi S, Tashiro K, Kitagawa K, Iwasaki Y, Abe H. A mechanism of juvenile muscular atrophy localized in the hand and forearm (Hirayama’s disease): Flexion myelopathy with tight dural canal in flexion. Clin Neurol (Tokyo) 1987;27:412-9.
- Jakhere S, Wagh V. Hirayama’s disease: The importance of flexion magnetic resonance imaging. J Postgrad Med 2011;57:48-50.
- Chen CJ, Hsu HL, Tseng YC, Lyu RK, Chen CM, Huang YC, et al. Hirayama fl exion myelopathy: Neutral-posi on MR imaging fi ndings – importance of loss of a achment. Radiology 2004;231:39-44.
- Gandhi D, Goyal M, Bourque PR, Jain R. Case 68: Hirayama disease. Radiology 2004;230:692-6.
- Mukai E, Matsuo T, Muto T, Takahashi A, Sobue I. Magnetic resonance imaging of juvenile-type distal and segmental muscular atrophy of the upper extremities. Rinsho Shinkeigaku 1987;27:99-107.
- Chiba S, Yonekura K, Nonaka M, Imai T, Matumoto H, Wada T. Advanced Hirayama disease with successful improvement of activities of daily living by opera ve reconstruction. Intern Med 2004;43:79-81.
test comment
By : Prajyotan B - On : 3/3/2018 5:18:00 PM